Sponsored by Hoechst Marion Roussel, Inc., makers of
Cardizem® Injectable 
Click here for information and a
free EKG Tutorial
Sponsored by Hoechst Marion Roussel, Inc., makers of
Cardizem® Injectable
Click here for information and a
free EKG Tutorial
Personal comments from the contributors (noninclusive, to be sure) are included.
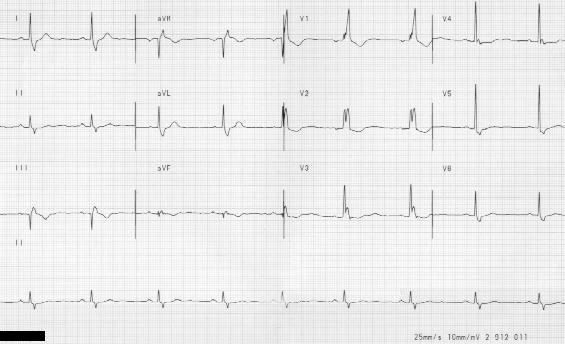
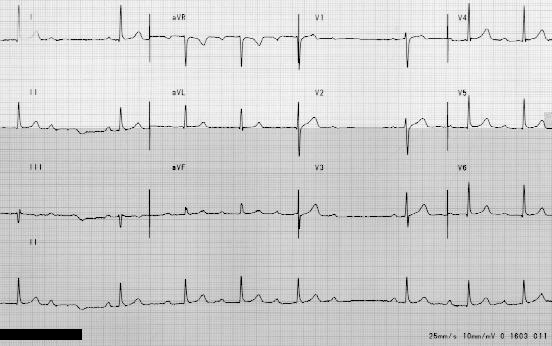
#6 Sinus rythm with right bundle branch block . Wide S in I, wide R in AVF, R to R' in right precodial leads." Dr. H. Nussbaum
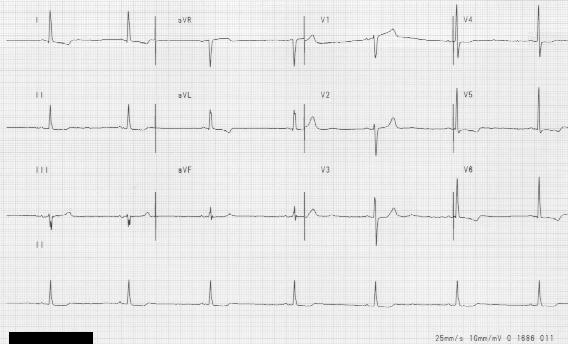
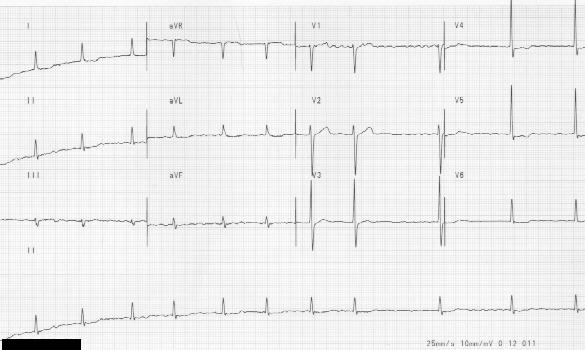
#10 Sinus bradycardia, rate below 50, regular rythm. The shallow T wave inversion in leads I, AVL, and the left precordial leads are due to left ventricular hypertrophy with repolarization effect." Dr. H. Nussbaum
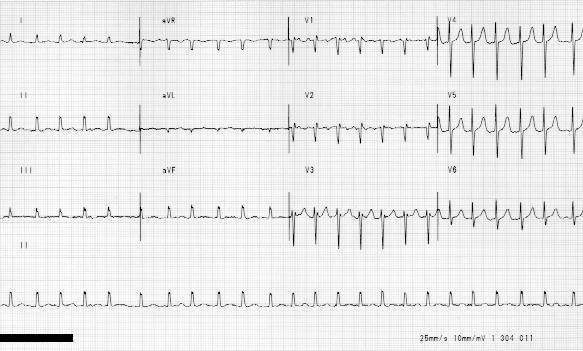
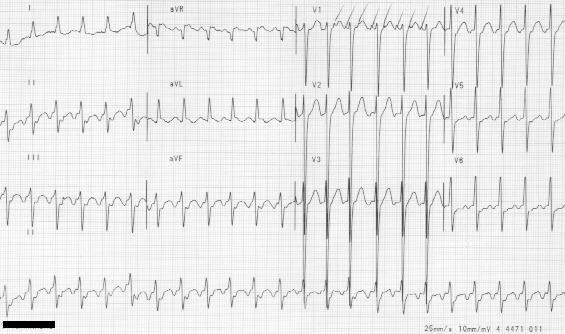
#3 Atrial fibrillation with rapid ventricular response . Dr. H. Nussbaum
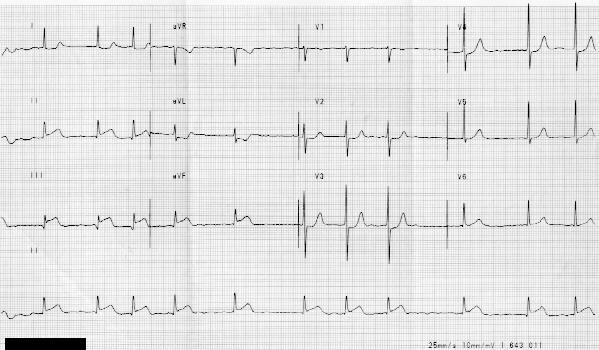
#12 Atrial fibrillation, acute inferior wall MI. "Totally irregular ventricular rythm and absent P waves, but with fibrillatory base. The patient also has an acute inferior wall infarction with Q waves in leads II, III, AVF, and elevated ST segments. The depressed STs in precordial leads are a reflection of the inferior lead elevations". Dr. H. Nussbaum
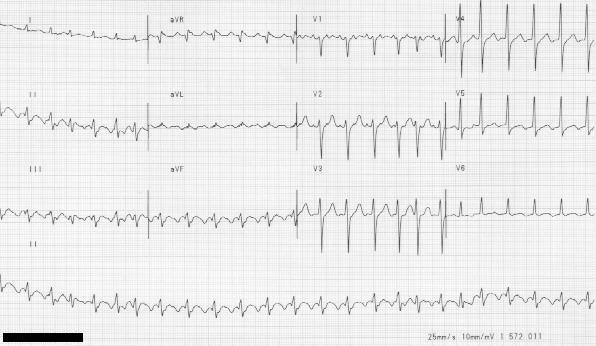
#18 Totally irregular rythm with absent P waves of atrial fibrillation . T waves are nonspecifically flat or shallowly inverted" Dr. H. Nussbaum
#23 A Fib. Dr. H. Nussbaum
#4 This is atrial flutter with 2:1 AV block, with blocked P waves seen best in V I . Dr. H. Nussbaum
#5a Atrial flutter with varying degrees of AV block. Dr. H. Nussbaum
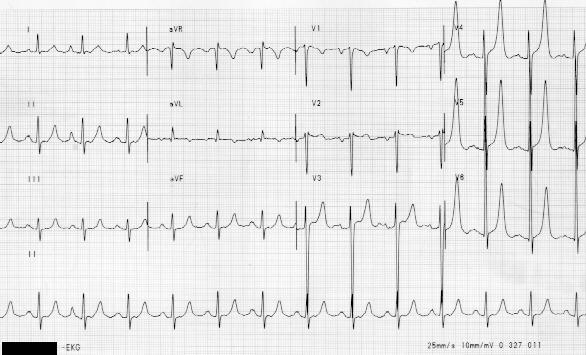
#9 Atrial flutter with 3:1 block. This tracing has a characteristic flutter wave baseline seen in leads II, III, AVF. Dr. H. Nussbaum
#13 Characteristic atrial flutter, with 2:1 AV block. The flutter rate is usually about 300 with a resulting ventriuclar rate of about 150 when 2:1 block exists. Dr. H. Nussbaum
#8 This is second degree AV block (Mobitz I), note progressive increase in the PR interval until a blocked P wave occurs. Also note the progressive shortening of the R-R interval. Dr. H. Nussbaum
#7 Complete AV block. There is no relationshiop between the P waves (atrial beats) and the ventricular beats. The latter rise from different foci. Some supraventicular beats with a RBBB configuration. Some ectopic beats in the ventricule. Dr. H. Nussbaum
#2 Left bundle branch block. QRS measures greater then 0.12 sec and has deeply negative QRS in right precordial leads. This type of EKG can deceptively hide an anterior wall myocardial infarction. Dr. H. Nussbausm
#21 "Sinus rythm, left axis deviation, wide QRS, LBBB, note inverted T waves in leads I, AVL in left precordial leads. The ST segment seems to slide off the QRS which is characteristic of LBBB with repolarization defect.Dr. H. Nussbaum
#6 Sinus bradycardia, RBBB . Dr. H. Nussbaum
#7 Complete AV block, RBBB . Dr. H. Nussbaum
#22 RBBB . Dr. H. Nussbaum
#12 Inf. Wall MI, A fib . Dr. H. Nussbaum
#17 With RBBB, old inferior wall MI. Anterior infarction in RBBB patient, the loss of the typical R to R' configuration in right precordial leads is due to the substitution of the Q wave of infarction. An old inferior infarction -note tiny R wavesnot unusual for old inferior infarctions "to regrow" small R waves. Dr. H. Nussbaum
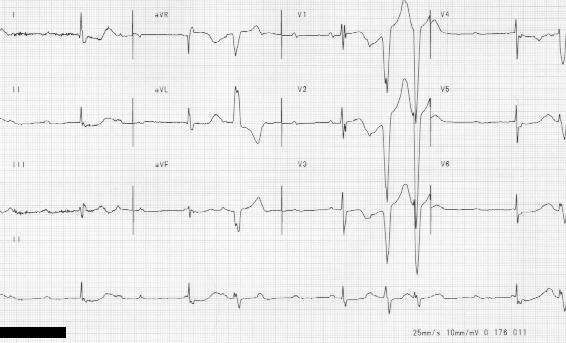
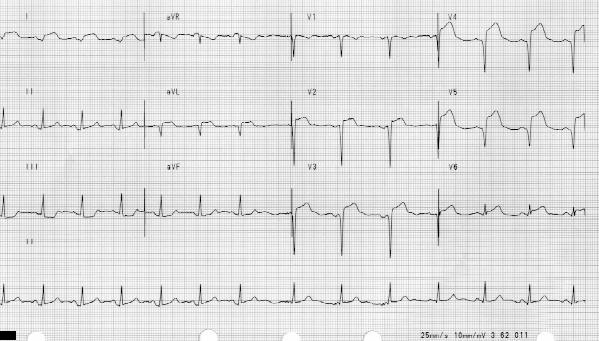
#19 Acute anterior wall MI, old inferior wall MI . Sinus rythm, Q wave in leads II, III, AVF , old inferior wall infarction, Q waves in precordial leads, VI- V6. Transmural anterior infarction with markedly elevated ST segments in precordial leads. Current of injury, a sign of acuteness of process. Dr. H. Nussbaum
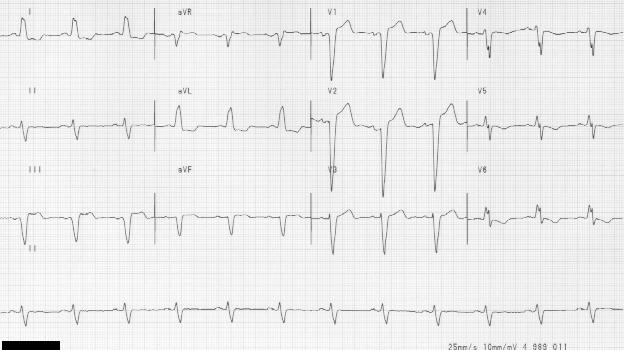
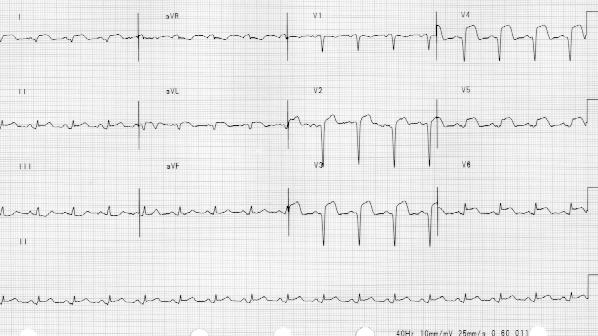
#20 Same patient as #19 one day later, except note evolution to inverted T waves in precordial leads. This is a further progression" Dr. H. Nussbaum
#24 Anterior wall MI @ 13:30 Dr. G. Fink
#25 Anterior wall MI @ 14:28 Dr. G. Fink
#26 Anterior wall MI @ 17:00 Dr. G. Fink
#27 Anterior wall MI @ 19:21 Dr. G. Fink
#28 Anterior wall MI two days later Dr. G. Fink
#14 hyperkalemia 17:01 Extensive evidence of hyperkalemia, note loss of P wave voltage, and dramatic increase in width of QRS complex> Dr. H. Nussbaum
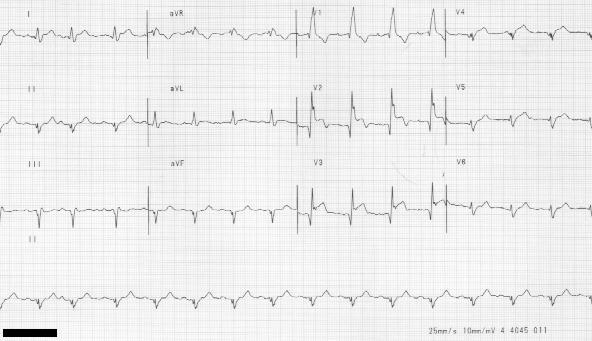
#15 hyperkalemia 23:46 This tracing follows 6 hours of therapy for hyperkalemia of #14 above, note normalization. Dr. H. Nussbaum
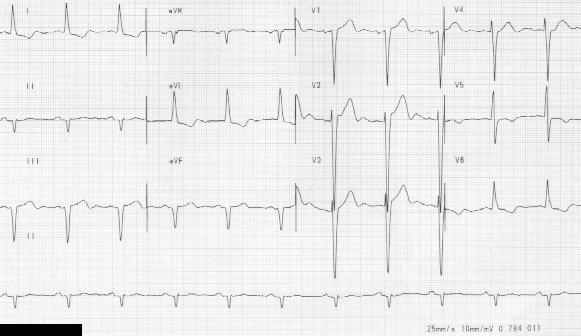
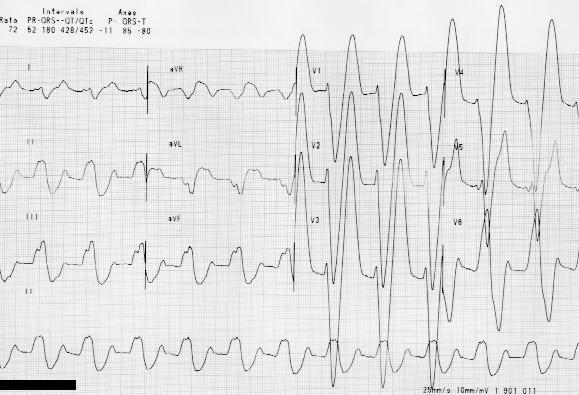
#16 hyperkalemia "Next day #15 above- note the configuration of the precordial T waves. They're sharply elevated with a peaked top and a narrow base characteristic of hyperkalemia. Hyperkalemia frequently exists without these classical findings. Dr. H. Nussbaum
Contributors:
Glenn D. Fink M.D.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}