Examination of the head and neck
Examination of the head
Inspection
Palpation
Percussion
Face
General inspection
Expression of the face
Innervation of the cranial nerves
Eyes and surroundings
Nose
Lips
Oral cavity
Ears
Examination of the neck
Inspection
Palpation
Auscultation
Examination
of the head
For systematic examination of the head, inspection, percussion, and
palpation is used.
Inspection
The head is usually mesocephalic in shape,
freely moveable, with a characteristic boundary between the facial
and hairy parts.
We recognise the following head shape variations:
Movement
is limited in meningeal irritation, when the head is buried into the pillow, the body is actually in opisthotonus (meningitis, meningoencephalitis, subarachnoid bleeding, meningism in pyretic conditions).
Shiver
Hair cover
has a characteristic boundary with the face, different in men and in women.
Alopecia (hairlessness) is the most common deviation.
Palpation
Deviations are usually not recognised by palpation of the hairy part of the head.
These conditions occur pathologically:
 |
Small tumours – usually smaller in size
|
||||||
| |
Pulsating formations corresponding to angioma | ||||||
| |
Inflammations
|

The 1st, 2nd, and 3rd branches of the trigeminal nerve not painful.
Sensitivity of the 1st and 2nd branches can be present in frontal and maxillary sinusitis, sensitivity of all three branches occurs in neuralgia of nervus trigeminus.
Percussion
Percussional examination of the head is not painful.
The pain is related to traumatic changes, inflammations of the paranasal cavities or may be of dental origin. The percussional sound of a broken bowl is present in fractures of skull bones.
Face
is symmetrical, the skin is pink, with no pathological changes.
Inflammations
Neoplasms
| |
Benign tumours:
|
||||||
| |
Malignant tumours:
|
"Butterfly exanthema" occurs in case of lupus erythematosus.
Swellings can be:
| |
Of dental origin |
| |
Above the maxillary cavities |
| |
In front of the ear, by the parotid gland |
Prominences: Most often xanthelasmata of the eyelids (hyperlipoproteinaemia, primary biliary cirrhosis, diabetes mellitus).
Hirsutism in older women around the mouth, pathologically in tumour of adrenal glands and ovaries with androgenic activity.

The expression
of the face
gives the information about patient’s mental condition, some characteristic
changes induce suspicion of severe illnesses.
Facies in cases of endocrinopathy
Innervation
of the cranial nerves
N. VII. (facialis) innervates facial muscles.
Central paresis - is expressed by unilateral
affection of the lower branch, i.e. by depression of the corner
of the mouth, smoothening of the nasolabial sulcus, inability
to purse the mouth or to whistle. It is often present in cerebral
apoplexy, or sometimes isolated without concurrent hemiparesis.
Peripheral paresis - is characterised by the unilateral
affection of both upper and lower branches. Asymmetry of the eye
slits, and inability to close the eye are typical for the upper
branch affection (the eye slit is wider). Eyeballs rotates externally
(Bell's symptom) in attempt to close the eye.
There is a danger of a corneal ulcer. The patient has smoothened
wrinkles and is unable to frown or to pull up the eyebrows.
N. V. (trigeminus) - see palpation of the head.

Facies mitralis

Polycytemia

Face of an
acromegalic

Hands of an
acromegalic
![]()
Legs of an
acromegalic

Cushingoid
facies
Eyes
and surroundings
Eyebrows are symmetrical, eyelids without swellings;
eyeballs are in the central position, freely moveable in all directions.
| |
Asymmetric eyebrows can be found in patients with congenital facial disorders, defects of innervation of the upper branch of n. VII (the patient is unable to frown or to raise the eyebrows). |
| |
Thinned eyebrows - in the temporal region in hypothyroidism. |
| |
Supraorbital arcs are thickened in acromegaly. |
Eyelids
Eye slits
| |
Bilateral narrowing occurs in blepharospasm. |
| |
Part of the sclera is visible above the iris when the examined eye is looking down (Graefe's phenomenon) |
| |
Asymmetry can be observed in unilateral ptosis of the eyelid (Bernard-Horner syndrome - ptosis, meiosis, enophthalmos in cervical sympathetic lesions). |
Eyeballs
| |
Exophthalmos represents a bilateral protrusion of the eyeballs in patients with thyrotoxicosis, or a unilateral one in retrobulbar lesions, tumours of the frontal skull fovea. |
| |
Enophthalmos is usually unilateral (see above). |
| |
Convergent strabismus – axes of the eyeballs converge (convergent squint). |
| |
Divergent strabismus – axes of the eyeballs diverge (divergent squint). |
Motility of the eyeballs:
| |
Convergent and divergent strabismus |
| |
Nystagmus represents unintentional, quickly repetitive, rhythmic movements (twitches) of the eyes of horizontal, vertical, or rotary type (vestibular syndromes). |
Conjunctivae are pink, sclerae are anicteric.
Conjunctivae
| |
Paleness is present in anaemia. |
| |
Hyperaemia in conjunctiva inflammation. |
| |
Xerophthalmia is present in keratoconjunctivitis sic´ca (Sjögren´s syndrome). |
Sclerae
| |
Yellow colour appears in icterus in hypercarotinemia. |
| |
Reddening of the bulbar conjunctiva occurs in conjunctivitis. |
| |
Sub-conjunctival haemorrhage is associated with bleeding, excessive exertion,sometimes the cause is unknown. |
Pupils
are round, isocoric, react to light exposure and convergence.
| |
Meiosis (narrowing) occurs after illumination of the eye, it can be found in some types of iris inflammation, in progressive paralysis, after administering pilocarpine into the eye, in glaucoma, in morphine intoxication, as a part of Horner's triad. |
| |
Mydriasis (dilatation) is a reaction of the eye to the dark. It can be observed in deep unconsciousness, in some types of CNS injuries, after atropine administration in the eye, in acute glaucoma, in amaurosis and in belladonna intoxication. |
| |
Anisocoria (different width of the irises on each side) is present in cerebral apoplexy. |
| |
Argyll-Roberts reaction means retained convergent reaction, but absent illumination reaction (neurolues). |
Cornea is transparent.
| |
Turbidities and ulcers occur after cauterisation, injuries, or inflammations (herpes zoster of the 1st branch of nervus trigeminus). |
| |
Arcus senilis lipoides corneae is a grey-white stripe on the edge of the cornea (fat deposit – seen in hyperlipoproteinaemia). |
| |
Corneal reflex is absent in deep unconsciousness. |
Nose
is of adequate size and shape, symmetric, freely passable, without secretion.
| |
Big nose is observed in the case of acromegaly. | ||||
| |
Rhinophyma is an enlarged nose, with rough surface (potato nose), especially in hypertrophic rosacea. | ||||
| |
Saddle nose is seen in cases of congenital syphilis. | ||||
| |
Asymmetric nose usually after injuries. | ||||
| |
Epistaxis (profuse nose bleeding) – after injuries, in cases of uncontrolled hypertension, in cases of haemorrhagic diathesis or rhinitis. | ||||
| |
Inflammation:
|
![]()
Swelling of the
upper eyelids +
anaemic aspect
in case of
nephrotic syndrome

Swelling of the
lower eyelids
![]()
Eyeglass-like
haematoma, abrasions
in the face
![]()
Gerontoxon
![]()
Gerontoxon,
arcus senilis
corneae
![]()
![]()
Xanthelasmata
of the upper and
lower eyelids
![]()
Ptosis of the
left eyelid
![]()
Oedema of the
upper eyelid and
eversion of the
lower eyelid of
the right eye,
asymmetry of the
eye slits
![]()
Divergent
strabismus
on the right side

Icterus of the
facial skin
![]()
Yellowish sclerae
![]()
Coloboma iridis
of the right eye,
post-operational
state
Lips
are symmetric, pink, smooth, and moist.
| |
Asymmetric lips - mouth corner is lowered, the patient is unable to purse the mouth or to whistle; usually observed in paresis of the lower branch of the facial nerve, sometimes the asymmetry is caused only by defective teeth. | ||||
| |
Cyanotic lips are present in faulty haemoglobin saturation by oxygen in patients with inborn heart defects, bronchopulmonary diseases. | ||||
| |
Dry lips occur with dehydration; sometimes crevices occur. | ||||
| |
Inflamed lips:
|
||||
| |
Anguli infectiosi occur in vitamin B2 deficiency, insufficient hygiene, and immunodeficiency. |
Oral cavity
Smell from oral cavity (foetor ex ore) is not normally present.
| |
Non-characteristic smell is present in case of infection in oral cavity (gingivitis), retention of food in decayed teeth, ulcer, tumour in the mouth, ENT area, oesophagus, or stomach, lung abscess and particularly gangrene of lung (intensive putrid smell). |
| |
Characteristic acetone smell is detectable in ketoacid hypoglycaemic coma. |
| |
Alcoholic smell occurs in alcohol intoxication, but also after drinking of little amount of alcohol (not so intensively). |
| |
Hepatic smell is presented in liver malfunction (the smell is similar to the smell of mice or fresh liver. |
| |
Urine smell occurs in renal malfunction (smell of ammonia). |
Mucous membrane of oral cavity is pink, shiny, without pathological changes.
Although it may be:
| |
Pale in anaemia. |
| |
Erythematous in stomatitis, sometimes together with apththae. |
| |
Black spots of melanin pigmentation occur in oral mucous membrane in Addison's disease. |
| |
Koplik's spots (yellow-whitish spots) occur in measles. |
| |
Petechia, suffusion occurs in case of haemorrhagic diathesis. |
| |
Erosion, ulcers are presented on mucous membrane in agranulocytosis or acute leukaemia. |
| |
Soor (thrush) – whitish fur on mucous membrane, it can be wiped off, it manifests in antibiotic therapy, mainly in elderly people, in immunodeficiency. |

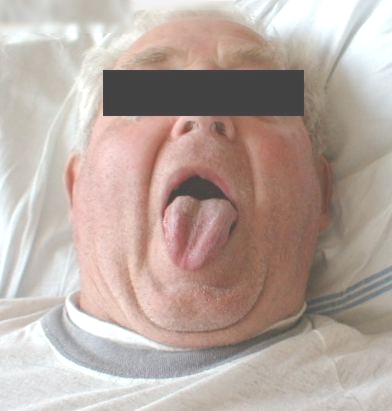
Tongue sticks out in medial line, it is pink and wet.
| |
Deviation occurs in cerebral apoplexy, when the healthy side pushes the tongue to the affected side. |
| |
Dry tongue is a manifestation of dehydration of organism in case of insufficient intake or enormous loss of fluid (vomiting, diarrhoea, fever), tongue dryes up after breathing through the mouth, or when production of saliva is decreased. This observation is very important for assessing the state of hydration of patient's organism! |
| |
Coated tongue is characteristic for the diseases of the oral cavity or systemic diseases. |
| |
Raspberry-coloured tongue occurs in scarlet fever after separating of the superficial fur. |
| |
Hunter's glossitis (extinct erythematous tongue with atrophic papillae) is a usual finding in pernicious anaemia. |
| |
Leucoplakia manifests as blue-white or silver-shiny stripes on the tongue surface, on buccal mucous membrane (pre-cancer state). |
| |
Bitten tongue at the tip or on the sides of tongue occurs in patients after big epileptic seizure (grand mal). |
| |
Macroglosia occurs in acromegaly, myxoedema, angioneurotic oedema, and glossitis. |
Gums are pink, strong, without bleeding signs.
| |
Erythematous, soaking gums are manifestation of gingivitis. |
| |
Bleeding signs are notable in C-hypovitaminosis (scurvy), periodontitis, or haemorrhagic diathesis. |
| |
Coloured edge of greyish colour originates in chronic intoxication by heavy metals (lead, bismuth). |
| |
Soor can be found usually on the border between buccal mucous membrane and gingiva. |
Teeth are fully developed, healthy.
| |
Decayed teeth can be the source of focal infection (lack of oral hygiene). |
| |
Defective teeth may cause difficulties in chewing, possibly a source of focal infection. |
| |
Dentures (prosthesis) – bad quality made prosthesis can cause chewing difficulties. |
| |
Periodontitis manifests by gingivitis, teeth loosening, formation of gingival grooves and sometimes abscesses. |
The pharynx entrance is symmetrical, mucous membrane is pink, symmetrically opening when phonating, and tonsils are symmetrical, partly submerged.
Soft palate, arches, uvula
| |
Yellowish or yellow palate - in earlier phase of icterus. |
| |
Erythematous - in respiratory infections. |
| |
Blisters – in viral infections. |
| |
Asymmetric - with overstretching into the healthy side in diphtheria. |
Tonsils
| |
Missing - state after tonsillectomy. |
| |
Submerged in adulthood and in old age (atrophy of lymphatic tissue). |
| |
Hypertrophied, with furrows, usually in chronic tonsillitis, sometimes with "presence of focuses". |
| |
Enlarged, erythematous, with furs - in acute tonsillitis. |
| |
Asymmetric, bulging in retrotonsillar abscess or tumour. |
Ears
are of a characteristic shape, external auditory canal without effusion; pressure on tragus and palpation on processus mastoideus are painless.
| |
Gouty tophi on auricle are yellowish subcutaneous deposits of urates. |
| |
Secretion in the auditory meatus occurs in case of meatus inflammation or otitis media. |
| |
Bleeding from the auditory meatus has usually a traumatic origin. |
| |
Pain when pulling the auricle, pressing on the tragus, and percussion onto processus mastoideus occur in case of otitis media or mastoiditis. |
Deviation of the
tongue to the
right side in
cerebral apoplexy

Dry tongue in
dehydration

Dry tongue in
dehydration
Examination
of the neck
In examining the neck, inspection, palpation, and auscultation is
used.
Inspection
The shape and length of neck are proportional to the body.
| |
Slim neck - appears in cachexia; the supraclavicular areas are notably sunken. |
| |
Strong neck - in obese people. |
| |
Pulsations of carotid arteries are visible in skinny people in exertion, hypertension, hyperthyreodism, and mainly in aortal insufficiency. |
| |
Horizontal scar – state after strumectomy, visible in fossa jugularis. |
Goitre, enlarged lymphatic nodes, and filling of neck veins is visible in pathological conditions described below.
Post-radiation changes on the skin of the neck are usually found after radiotherapy of malignant tumours.
Movement is free in all directions.
Movement limitation occurs in vertebrogenic syndromes, meningeal irritation, Bechterev's disease, torticolis spastica (tonic contracture of musculus sternocleidomastoideus).
Musset's symptom displays abnormal movement of head and neck in aortal insufficiency.
Change of posture
| |
Deviation to the side – result of bleeding into the neck muscles, muscle rupture, fibrositis, or reflex spasm of muscles. |
| |
Opisthotonus – inversion to the back in case of tetanus. |
Palpation
Carotid artery
Weakened or not palpable pulsation indicates contraction or complete obstruction of the vessel lumen.
Thyroid gland is normally neither visible nor palpable. The enlargement of the gland is called goitre – diffuse or nodal.
| |
Small diffuse goitre, bilaterally slightly enlarged, has a soft consistency (eufunctional goitre in adolescence). |
| |
Colloidal goitre is usually diffuse, symmetrical, has a more rigid consistency, (occurs in adulthood, usually eufunctional). |
| |
Hashimoto's goitre has usually more rigid consistency, rough surface, with signs of hypothyroidism (auto-immune disease). |
| |
In case of thyroiditis thyroid gland is slightly enlarged, spontaneously and mainly palpation-sensitive, hyperfunctional at the beginning, progresses to hypofunction. |
| |
Basedow's goitre is diffuse, bilaterally enlarged, symmetrical, elastic, soft, pertinently with palpable whirl and audible murmur (puff). |
| |
Malignant goitre is markedly rigid, very sensitive to palpation, of limited potential to be move, often fixed to the base, rapidly progresses. |
| |
Nodal goitre where one lobe or its part is affected appears clinically as eufunctional or hypofunctional. |
| |
Retrosternal goitre – enlarged thyroid gland reaches behind the sternum, sometimes visible on the neck, its function may be normal, but can cause mechanical problems. |
Cervical veins – in healthy lying patient with elevation of the upper part of trunk at 45 degrees, the filling of the veins does not exceed the horizontal level of sternocostal joint for more than 2 cm.
| |
Increased filling is a sign of venostasis in front of the right heart, it manifests in right heart insufficiency, constrictive and exudative pericarditis, tricuspidal valve disorders. |
| |
Positive vein pulsation is obvious in insufficiency of tricuspidal valve. |
| |
Hepatojugular reflux demonstrates an increased pressure in cervical veins persisting for the time of firm pressing the liver with the flat hand (30 – 60 seconds). Originates in right heart insufficiency and insufficiency of tricuspid valve. In healthy individuals it occurs only at the beginning of the examination. |
| |
Stokes collar occurs in venostasis in the head and neck area, its main signs are oedema and cyanosis. It is most often caused by tumorous compressing vena cava superior. |
Regional lymphatic nodes are not visible or palpable. In examining their size, rigidity, painfulness, demarcation, fixation to the base and localisation are observed. The most common findings are:
| |
Enlargement of inflamed node
|
||||
| |
Enlargement of tumorous node
|
Auscultation
is used in examination of the carotids. Presence of systolic murmur indicates possible sound propagation from aortal orifice (bilateral audibility) or carotid artery stenosis (asymmetric audibility of the murmur).
The murmur can also be audible above the Basedow's goitre.
Your notes, observations, and proposals are welcome either via e-mail at the address

Scar after
strumectomy
![]()
Post-radiation
changes on the
neck surface

Phlegmon of the
neck (state after
punctue)
![]()
Polynodose
goitre