Thorax examination
Orientation on the thorax
Observation
Palpation
Percussion
Auscultation
Most common physical medical findings in airway disorders
Acute bronchitis
Lung emphysema
Pleural exudate
Types of exudates
Pneumothorax
Crupous pneumonia
Atelectasis
Bronchopneumonia
Asthmatic attack
Breast examination
is performed by the means of observation, palpation, percussion, and auscultation.
Orientation on the thorax

Front:
1. Anterior medial line - in the middle of the sternum.
2. Sternal line - around the edge of the sternum.
3. Parasternal line - between the sternal and medioclavicular lines.
4. Medioclavicular line - in the middle of the clavicle.
Side (5):
Anterior axillar line - around the lateral edge of m. pectoralis
major.
Middle axillar line - in the middle of the axilla.
Posterior axillar line - around the lateral edge of m. latissimus dorsi.
Back:
(6) Scapular line - horizontal line through the inferior
angle of the scapula.
(7) Paravertebral line - around
the edge of the vertebral column.
(8) Back medial
line - in the middle of the vertebral column following
spinous processes.


Observation
A normal thorax is symmetrical, widening evenly with breathing.
It is necessary to notice possible breathlessness, cyanosis, or painful breathing before starting the physical examination.
Shape variations of the thorax:
During examination, it is possible to notice kyphosis or kyphoscoliosis.
Post-operative scars after thoracotomy (lung and heart surgery) should also
be noted.
Breathing
Eupnoea means normal breathing with a frequency of 16 - 18 breaths per minute.
Palpation
Of the thoracic wall is used mainly for detection: of thoracic vibrations,
a pleural frictional murmur, a quality of thoracic wall, tenderness,
and resistance.
Thoracic vibrations (fremitus pectoralis) are normally symmetrical on both halves of the thorax.
A pleural frictional murmur can be palpable in patients with severe dry pleuritis.


Kyphoscoliosis,
gibbus

Fresh scar after
sternotomy

Older scar after
sternotomy
Percussion
In healthy person it is full, bright, comparable on both halves of the thorax.
Auscultation
Under physiological circumstances, clear alveolar breathing is present over the lungs, without any side phenomena. Tubal breathing can only be heard over the upper sternum and between the scapulae.
Alveolar breathing
| |
Sharpened diffusely - during increased breathing, e.g. acidotic breathing (decompensated diabetes mellitus, uraemia). unilaterally - compensatory manifestation (broad infiltration, compression by fluidothorax). |
| |
Weakened - present with emphysema, atelectasis, pleural exudate, and pneumothorax. |
| |
With prolonged expiration - occurs in airway obstruction (chronic obstructive bronchopulmonary disease, bronchial asthma) |
| |
Mixed - can be present in bronchopneumonia. |
Tubal breathing
If heard outside the major airways, it is a pathological finding. It is caused by exudation to alveoli (pneumonia) or by their compression (exudate).
Side breathing noises
| |
Dry noises - whistling, squeaking, or crackling; arising from vibrations of the viscous secretions during both inspiration and expiration. They occur with acute and chronic bronchitis and bronchial asthma. The findings vary in connection with cough. | ||||||
| |
Wet noises - occur in presence
of a liquid or semi-liquid content in the airways.
|
||||||
| |
Pleural frictional murmur - squeaky sound caused by the friction of inflamed pleural layers. It is detected in case of dry pleuritis. |

Pectoral voice (bronchophony)
Can be heard evenly over the lungs:
| |
Weakened - arises from disorders of the air supply (atelectasis), exudate or pneumothorax. |
| |
Strengthened - is found in cases of lung infiltration (pneumonia, lung infarction). |
The most common physical findings in airway disorders
(examination description keeps the order of observation, palpation, percussion, and auscultation).
Acute bronchitis (a young man)
No breathlessness.
Distant bronchitic phenomena (can be heard in case of a large finding).
Fremitus pectoralis normal on both sides.
Percussion full and bright.
Alveolar breathing, in both phases there are either dry or wet phenomena present (it depends on intraluminal content).
Bronchophony unchanged.
Emphysema
Barrel-shaped thorax.
Fremitus pectoralis weakened.
Percussion hypersonic.
Breathing alveolar, weakened. If there is a chronic bronchitis present, the dry or wet phenomena are often heard.
Bronchophony weakened.

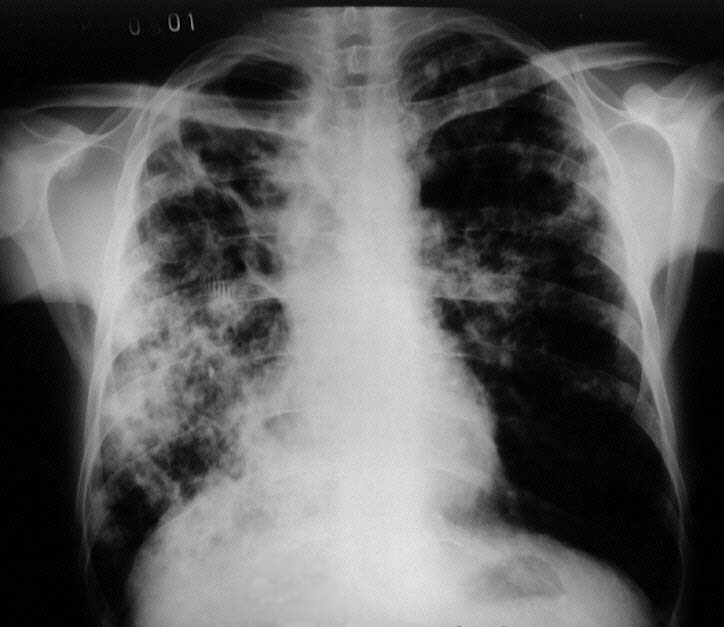
Pleural
exudate
Presence of fluid between the two pleural layers. It can be detected
when the volume exceeds 500 ml.
Usually without breathlessness, but it depends on the size of the exudate.
Fremitus pectoralis weakened in the area of exudate.
Percussion shortened or even obscured, exudate borders
have parabolic shape with the top in axilla. Near the upper
edge the percussion is hypersonic or even tympanal (skodaic
resonance).
Bronchophony weakened.
Types of exudates according to aetiology:
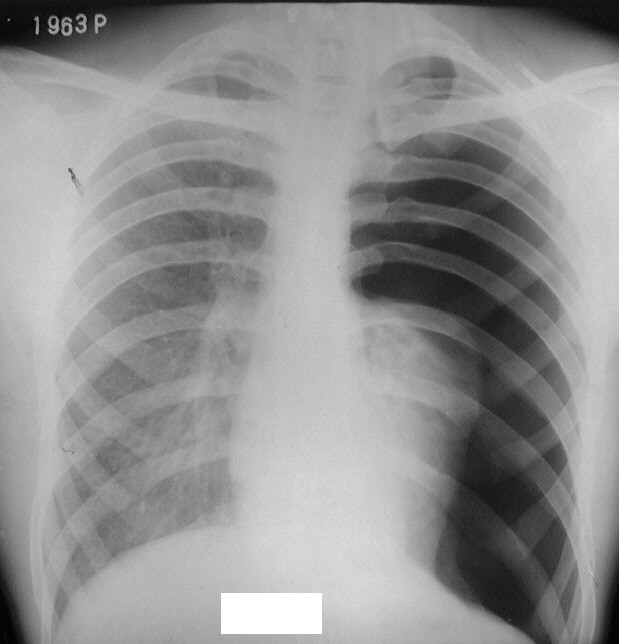
Pneumothorax
presence of air in the pleural cavity (trauma, rupture of emphysematous
bulla, iatrogenic origin).
Breathlessness depends on the size and cause of the pneumothorax.
Limited breathing movements of the affected thorax half.
Fremitus pectoralis weakened or missing.
Percussion hypersonic.
Breathing weakened or missing if the lung is completely collapsed.
Bronchophony weakened.
Atelectasis
means loss of air supply to alveoli, bronchi, bronchioles, or the whole
lung. The extend of affection depends on its cause.
In case of larger atelectasis breathlessness and cyanosis is present.
Fremitus pectoralis weakened.
Percussion shortened.
Breathing shortened.
Bronchophony weakened.
Pneumonia
(croupous)
The finding described below is seen only rarely in clinical practice,
because of current antibiotic treatment.
Breathlessness (may be manifested).
Fremitus pectoralis strengthened.
Percussion shortened.
Initially, crepitations are audible (crepitus indux), later tubal breathing
(phase of hepatisation), crepitations again (crepitus redux during resorbence),
progressive weakening of tubal breathing.
Bronchophony strengthened.
Bronchopneumonia
Breathlessness (may be present; it depends on the age and volume
of affection).
Fremitus pectoralis strengthened.
Crepitations and accentual noises can be audible.
Bronchophony is strengthened over the affection.
Asthmatic
attack
Orthopneic position, inspiratory position of thorax, severe expiratory
breathlessness, distress, and non-productive cough.
Fremitus pectoralis weakened.
Percussion hypersonic, lowered lung borders.
Audible distant bronchitic phenomena.
Prolonged expiration with numerous whistles and squeaks. They can often
be heard also during inspiration.
Bronchophony is diffusely weakened.
Examination
of breasts
Observation
| |
Symmetry and size of the breasts. |
| |
Appearance of the skin - reddening, retraction, and ridging. |
| |
Appearance of the nipples - impaction, purulent secretion (inflammation), or secretion containing blood (tumour). |
Palpation: local change of consistency – focus, its shape, size, border, and mobility:
| |
Oval with clear demarcation – suspected cysts. |
| |
Irregular, without clear demarcation and immoveable – suspect tumours. |
Your notes, observations, and proposals are welcome either via e-mail at the address