Examination of extremities
Oedemas
Digits (fingers, toes)
Nails
Skin
Muscles
Vessels
Joints
Extremities are symmetrical, without oedemas and skin disorders, well supplied with blood, and freely mobile.
Further described changes generally occur in lower extremities.
Oedemas


Oedema of lower
extremities
![]()
Cardiac oedemas
of lower
extremities

Shrunken skin
in lower
extremities
after the decline
of oedemas

Lymphoedema
of lower
extremity
![]()
Lymphoedema
of lower
extremity -
detail
![]()
Bilateral
lymphoedema
(congenital)

Lymphoedema
of lower
extremity
Deep venous
thrombosis

Obesity,
phlebo-thrombosis
of the left arm
Digits
Digits of upper as well as lower extremities are axially symmetrical, nails slightly arched, smooth, firm, with proportional representation of the lunula.
Clubbed distended digits with spherical nails, mostly cyanotic, occur in congenital cardiac defects and bronchopulmonary diseases.
Amputated - they are ablated (onycho-ectomy) usually due to serious ischaemic changes in diabetic patients or in ischaemic vascular disease of lower extremities.

Detail -
digital clubbing
in congenital
cardiac effect

Digital clubbing -
central cyanosis

Digital clubbing
in lower
extremity

Condition after
amputation of toes
(diabetic
microangiopathy)

Amputated toes
in a diabetic
patient
Nails
Koilonychia (spoon nails) - occur in thyrotoxicosis.
Cera guttans - lengthwise grooving alternated
with shallow depressions. These changes are present in rheumatoid
arthritis.
Onychomycosis - is manifested with uneven, friable
nails, changed in colour, single or multiple nails are affected, mostly
in lower extremities.
Hepatic - whitish part of
the nail (lunula) occupies a substantial part, can be found
in patients with liver cirrhosis.
Splinter haematomas - occur
in chronic infectious endocarditis (embolisation).

Onychomycosis
of the big toe
of the right foot

Splinter
haematomas
Skin
Skin on the extremities is pink, warm, firm, elastic with retained
skin appendices (adnexa).
Trophic changes - the skin is drier, colder,
desquamated, hair scarce or absent, presence of skin defects (ischaemic
vascular disease of lower extremities, diabetic angiopathy).
Changes in colour

Ischaemic
disease of lower
extremities -
dry necrosis
of the big toe

Ischaemic
disease of lower
extremities

Cyanosis,
ischaemia
![]()
Dry gangrene
of the big toe

Microbial eczema
in the area of
chronic vascular
insufficiency

Hyperpigmentation
of the crura

Palmar
erythema
Varixes are manifested as single bluish transparent subcutaneous nodes or as stem varicosity of v. saphena magna (great saphenous vein). Its filling is increased in standing position. Erythema (reddening) of the skin above them and the infiltrate following the course of the vein, is a manifestation of thrombophlebitis.
Inflammatory changes

Crural ulcer

Crural ulcer
![]()
Venous varixes

Erythema nodosum
in legs

Erythema nodosum
in legs

Psoriasis
in the crura

Dupuytren's
contracture,
palmar erythema,
tattooing on the
forearm

Dupuytren's
contractures

Keratoma palmare


Musculature
The muscles of extremities are proportionately developed, symmetrical with adequate muscular tonus.
Muscular atrophy - of a small or greater extent is developed in an inactive limb (immobility in vascular cerebral emergencies, in lack of movement due painful articular syndrome, etc.).
Muscular hypertrophy - occurs in atypical exertion of the limb (orthopaedic defects, paresis).
Vessels - arteries
Arterial pulsation is well palpable in typical localisations.
Reduced pulsation signals narrowing of the lumen, most often due to an arteriosclerotic plaque or thrombus.
Palpation is used for examination of a. femoralis, a. poplitea, a. dorsalis and a. tibialis posterior. Ischaemic changes develop in accordance with the severity of circulation disorder.
More detailed information on blood supply is provided by Doppler ultrasonography of the malleolar pressure (physiological finding is by 10 to 30 mm Hg higher compared to the arm).

Scars after
venous grafts
withdrawal

Scar in the
left arm
![]()
Scars after
venous grafts
withdrawal
Joints
Visible joints are of proper sublime shape, freely mobile.
Deformation of a joint is caused by the presence
of osteophytes, exostoses; the movement is reduced, scratching sounds
(knee, astragalus) can be heard on palpation.
Heberden´s nodes represent arthritis of the distal
interphalangeal joints.
Bouchard´s nodes affect the proximal interphalangeal
joints, which are irregularly roughened.
Halluces valgi a deformation of the 1st
metatarsophalangeal joint of the foot with deviation of toes (occur
in pes planus, improper shoes, or in genetic disposition).
Spindle-shaped (fusiform) swelling (intumescentia) of the joint
is caused by an inflammation. Frequent affection is found in proximal
interphalangeal joints in rheumatoid arthritis. Chronic
character of the disease causes ulnar deviations, later desaxations,
in the worst case even articular ankyloses. Interosseous hand muscles
are atrophic.
Gout related tophi look like whitish nodules
over joints of hands. They are caused by deposition of uric acid crystals
(gout).
Your notes, observations, and proposals are welcome either via e-mail at the address
![]()
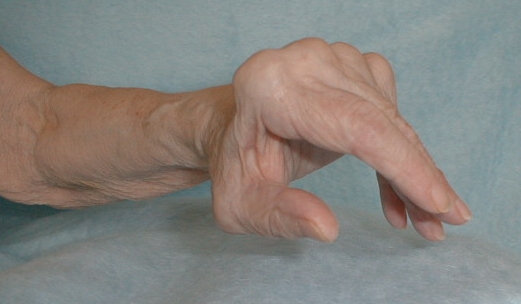
Deformation of the
wrist of the
right upper
extremity afer
Colles' fracture
![]()
Revmatoid
arthritis

Revmatoid
arthritis

Polyarthritis
of the hand -
gouty tophus